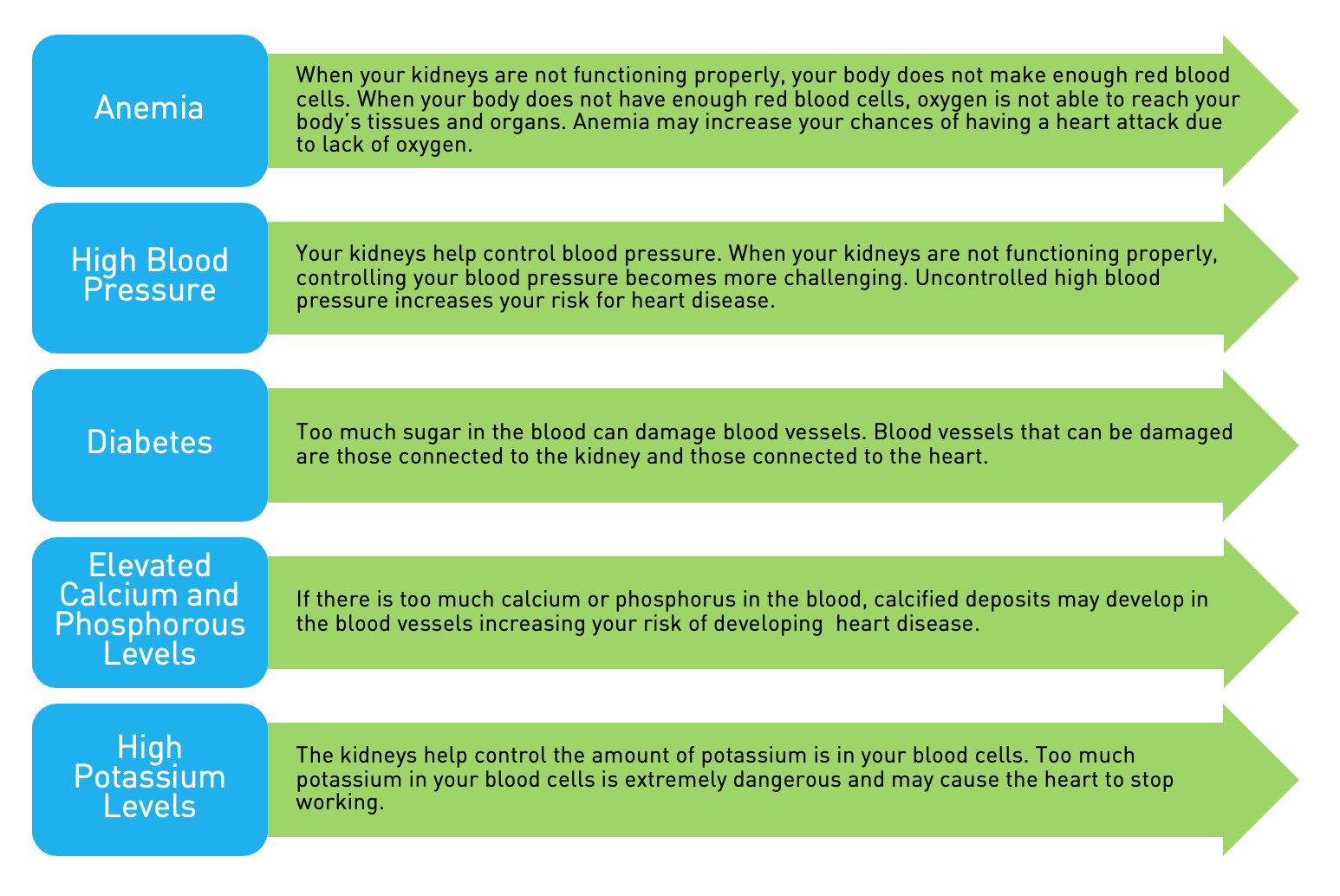
What is anemia and how is it managed in chronic kidney disease (CKD) before dialysis and after dialysis?
Anemia is a disorder where the body does not have enough red blood cells. Red blood cells are necessary because they carry oxygen from the lungs to the body tissues and carry carbon dioxide back to the lungs, where it is exhaled. The body tissues must have this oxygen in order to produce enough energy to function properly. The chemical processes which the cells use to make energy produce a molecule known as carbon dioxide which must be removed. The red blood cells have a second job – they stop extra acids in the body.
How does my body make red blood cells?
The red blood cells started out as stem cells that went through a growth process. There are hormones produced in the body that help stir-up this growth process. One of these hormones is erythropoietin.
Why do kidney disease patients have anemia?
Since erythropoietin is produced in the kidney, patients who have CKD may not produce enough.
What tests are used to manage anemia and what do they mean?
Your doctor will take several tests on a regular basis. These tests help determine how to best manage your anemia.
•CBC – Complete blood count – includes not just the hemoglobin, but also the white blood count and often the platelet count. It also has information that help doctors understand how much red blood cells you have. Large cells may show a lack in folic acid or B12. Small cells (microcytes) may show little iron in the system, chronic disease or a family disorder. The white cells can show infection and may show inflammation. The platelets are very important for blood clotting. This test is measured monthly in dialysis patients. If it is not normal, then additional tests may be needed.
•Hemoglobin – Hemoglobin is a molecule that contains iron. Iron has a very strong attraction for oxygen and is a perfect element for this purpose. The current range for hemoglobin is between 10 and 12 grams. The hematocrit is a ratio of red cells to blood and can be gathered by separating a small amount of blood. It is generally three times (3X) the hemoglobin level. Currently, the hemoglobin is measured and reported instead of the hematocrit.
•Iron – We are able to measure iron in the body. If the iron stores are low, the red blood cells cannot work properly.
•Iron saturation – The body is designed in such a way that iron I complexed to other molecules and closely controlled. It may be tied up in other tissues until it can be prepared for release. This makes it safer for the body. Iron can drive toxic reactions, too. In addition, iron is used by bacteria as well as by us. Therefore when one has a serious infection, the body tries to protect free iron and has ways to keep it away from these dangerous little organisms.
•Ferritin – Iron can also be stored in ferritin. These are another storage site helping to understand the total amount of iron in your system. Normal ferritins are around 100 to 300. Ferritin can be stored in the liver and the spleen.
What can I do to control my anemia?
First of all, anemia can have many causes. Kidney patients have little erythropoietin.
You may be short of certain support molecules like folic acid and B12 that can either directly cause you to have anemia, or contribute to it. You may also have either a slow or a rapid blood loss that can cause anemia. These items must be working well for the red blood cell process to work properly. Each month or so, many tests are measured during dialysis treatments and your health care team will go over these results with you while on dialysis. Home dialysis patients will have these explained during their monthly visits, so you can be kept up to date about how your anemia management is going.
You will be treated with an erythropoiesis stimulating agent (ESA), with iron, or both. ESAs are genetically engineered synthetics that work like erythropoietin. They are currently given intravenously or subcutaneously (under the skin) during your treatment. Examples include EPO or epogen, darbepoietin or Procrit. There are newer drugs that are also available. All of these drugs do the same thing – activate bone marrow to make red cells grow.
Iron can also be given through IV when on dialysis, depending upon your iron stores. Many patients need a maintenance dose each month. The AAKP Patient Plan booklets have been updated to reflect newer guidelines and management strategies for anemia. They are an excellent resource and can be found on the AAKP website, www.aakp.org.
Stephen Z. Fadem, MD, is a practicing Houston nephrologist and a Clinical Professor of Medicine at Baylor College of medicine. Dr. Fadem is Co-Chair of the AAKP Medical Advisory Board and Co-Medical Editor of aakpRENALIFE magazine.